This post is really a
display of the research I've been doing to find sites, and a beginning to each site's analysis. My post for Wednesday will return to the design and architecturing of the condition based on the information here and the decisions I made in this post. I KNOW I need to show you a lot of the things I describe in this text, and I WILL, but this is sort of brainstorming, analysis of what I've figured out, and the game plan.
I want to advance the idea of a healthcare system that infects civilization in the same way that AIDS has infected its populations.
A challenge I am working to address is defining the hierarchy, both architecturally and programmatically. What are the functions of the network at a series of scales?
The final and, I think, the most important challenge is picking a site or series of sites to focus on for the purposes of this project. The purpose would be to observe the system as it could exist in a variety of situations - its ability to adapt to the diverse socioeconomic, transportational, and need-based dilemmas that exist in the world is key in the proposal being successful.
_________________
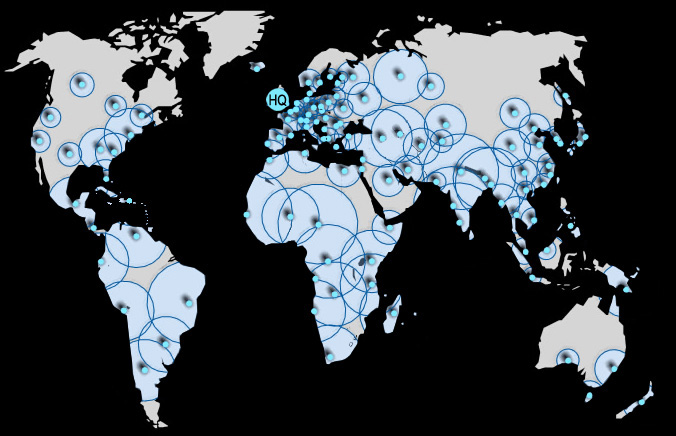
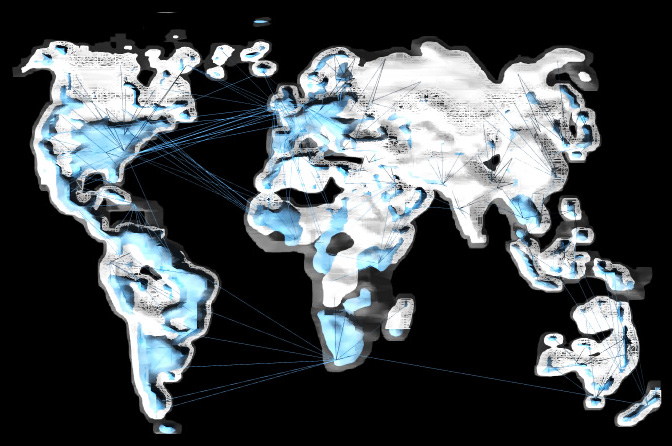
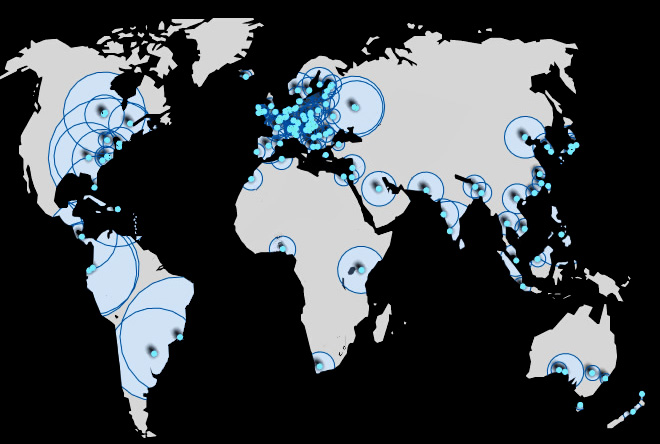
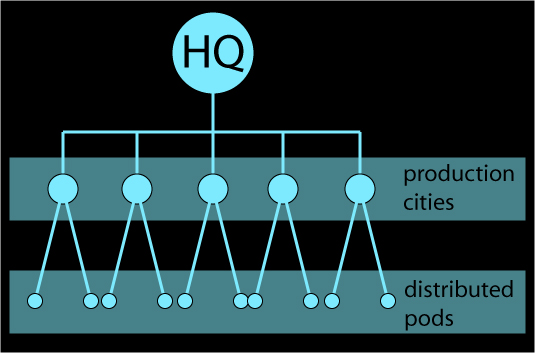
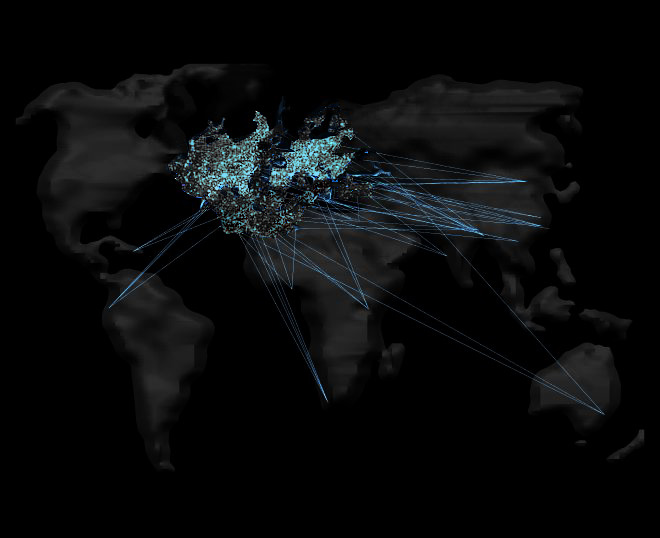
I. THE HIERARCHYPreviously, I had posted
this image to describe the corporate hierarchy of GSK as a network. I'm going to stick to that general concept, except instead of "distribution cities" they will be "hubs," meaning that they will contain a manufacturing and distribution plant but it does not necessarily mean a city. I'll examine in further detail.
What
HQ in London contains is the
knowledge, the
process (
and patents), and the
technology to produce lamiduvine and zidovudine. London distributes these things to the separate hubs in the chosen locations. This network is virtual; it purely exists within communicative means.
The
hubs contain these items which apply the virtual materials acquired from London, the
production of drugs, and the
production of the pods and the equipment they involve. The hubs are the plants that not only produce the treatments themselves, but they produce their methods and means, the architecture that allows the drugs to serve their purpose. It is these hubs that convert the virtual materials into physical, functional materials. The hubs will also help knowledge to build, because they will also contain
research which will gain knowledge that will travel both back to the HQ and will filter down to the pods.
The wellness
pods are containers that can be installed in a certain simple framework - a framework that can be expanded upon as needed and a framework that is minimally invasive. The programs of these pods include: 1. a portable
pharmacy (supplying an area with the needed drugs to treat its AIDS victims, see this previously posted
image). 2. A portable
doctor's office (or testing lab) which will be a room that can be either set in a remote village in order to test the population for AIDS, or it can be transferred to and installed within hospitals to function as an AIDS wing or AIDS section of the hospital. 3. A portable
hospital room for those extremely ill or dying or an AIDS-related infection, willing to pay extra to have the treatment and room in the comfort of their own homes (see
this image from the previous post). 4. A portable
information center to educate the uneducated populations on what AIDS is, how it gets contracted, and providing birth control education and STI education.
_________________
II. THE SITES
I defined the criteria for selecting manufacturing sites to this: central locations of transportation networks in their regions, areas with ample population to support and contribute to the functioning of these hubs, and regions where there is a need for AIDS treatment.
I've chosen the following sites to use as examples of a hub infecting a city.
Hyderabad, India is a logical site for a hub because it is located in a region where there is a high demand for AIDS medication, and it is a center for rail transportation in India, which is one of the main modes of transportation and shipment in India. There is also an airport in Hyderabad, which could provide an extra mode of access.
major railways in India
in relation to Hyderabad
Capetown, South Africa is a center for transportation in South Africa, and also has a port which opens up new routes of transportation and distribution for AIDS treatment. It is located in close proximity to poor areas, and the port access opens up the opportunity to ship the supplies up the coast to some of the other areas in dire need of treatment. In addition to rail and port, Capetown is one of the few cities in southern Africa with an airport.
major highways and railways of South Africa
in relation to Cape Town
The beauty of the pod is that it can be transported and applied virtually anywhere. The following are some recipients of pods that I will use as diverse examples of how they can be applied and implemented.
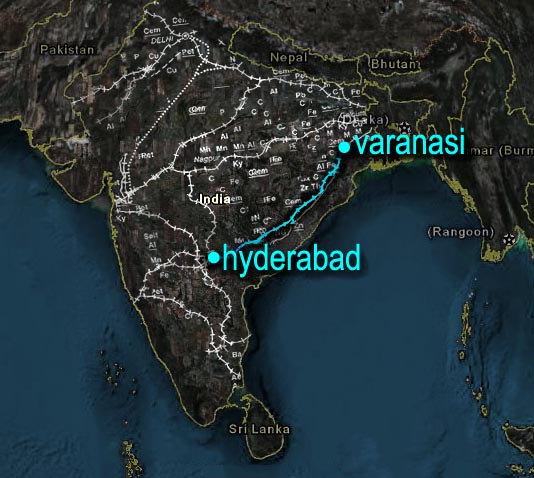
Varanasi, India is one of the larger cities in India, but the crime and poverty rate are higher than the other developed cities of India. The AIDS pandemic has struck Varanasi and its surrounding towns and villages harder than the rest of India. Class separation is evident, and while health technology is up-to-date, it reaches only the fortunate few. The economy is based around ancient crafts with a few cutting-edge institutions such as Texas Instruments plants and international universities placed within its boundaries. It is connected to Hyderabad by rail.
the route the treatment would take
from Hyderabad to Varanasi
Maseru, Lesotho is the capital of Lesotho. It is a small city of about 180,000, and is primarily comprised of low to middle class dwellings and a high unemployment rate. There is ample transportational access; it is located on the Caledon River (see map) which incidentally also runs through Capetown. There is a small international airport here, and two major highways run through it.
Omusati, Namibia is a region of Namibia with ample access to the Namibian port city of Skeletkuste. Transportation is extremely underdeveloped here, except for a massive freight road stretching across this northern wilderness. The healthcare system in this region is adequate at best; basic healthcare can be found but hospitals are few and underfunded. Like Maseru, it can be served by Cape Town as a hub.
the path treatment would take from Cape Town
to Maseru and Omusati
_________________
III. OTHER AFFECTING NETWORKSThe GSK network is going to exist as a supplement to already present conditions in each location. At every site containing the location of a hub, the transportation methods and networks would be mapped and the GSK network would latch on - using the existing transportation conditions as a means transport these pods.
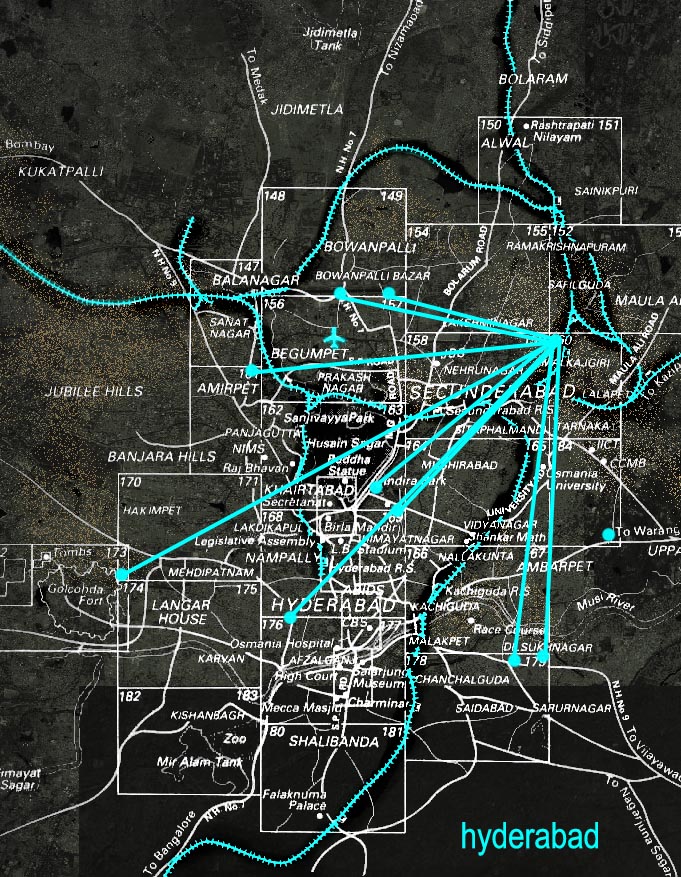
Hospitals that are already present - whether in cities, towns, or missionary hospitals in distant villages - will be mapped, and an AIDS wing will be made up of the aforementioned framework and placed alongside hospitals. In hub locations, the hub structures may exist as part of the hospital or an addition onto the hospital.Here I am zooming in a bit, and I've mapped the big transportation (mostly rails, that leave the city) and marked the significant hospitals.
Here I show the healthcare in Hyderabad as a network - making the hospital closest to the railroad leading to Varanasi the center of this mini-network. Perhaps this is how the GSK system can first invade the city at this point and attach onto the other hospitals via transportation, as an intra-city network.
I plan to do this level of analysis with all sites, whether they are hubs or not.
_________________
VI. FORMAL IDEAS
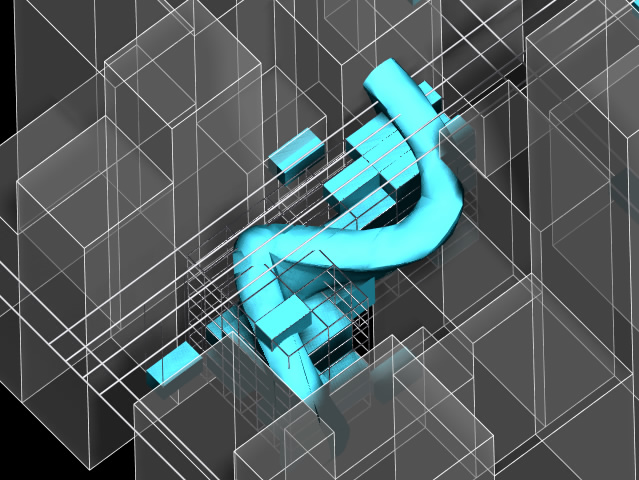
I found
this video of the AIDS virus infecting a human lymphocyte (white blood cell). What is happening in this video, is that the clump of cells starting out at the bottom have already been infected by the AIDS virus and are attacking the lymphocyte in the middle, violating the cell wall and causing the lymphocyte's insides to come out, a process called lysing (it pays to have biologically smart friends).
Architecturally, I would like the GSK network to act as a counter-infection on the population. In the same way that the virus enters a lymphocyte, takes control of it, and causes it to attack other lymphocytes, I want the architecture to infiltrate the population, take over, and spread. My idea for this is a collapsable, expandable, and multipliable structural system.
Stay tuned for more!






















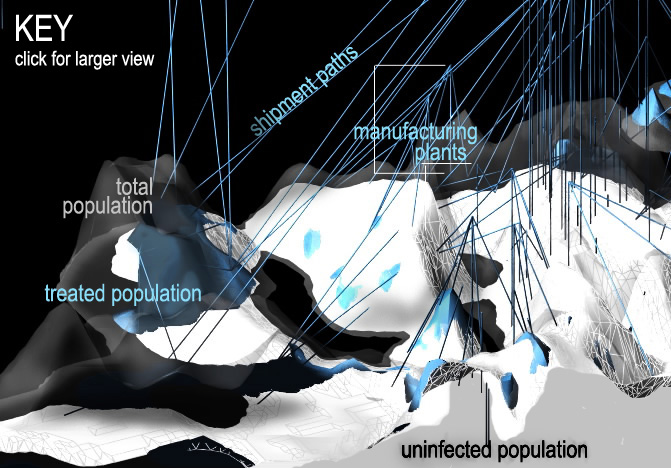
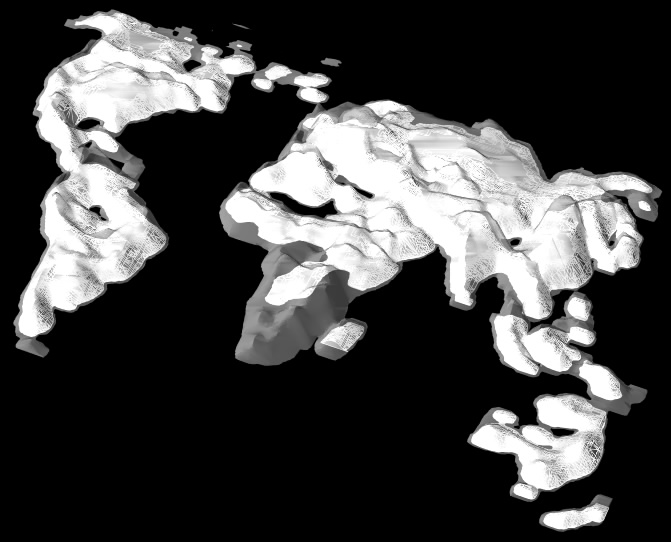



 solar heat absorption map
solar heat absorption map

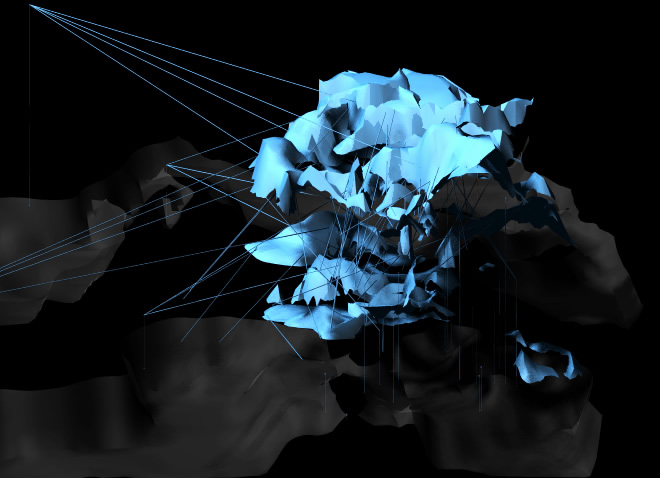
 solar heat absorption as a treated megaContinent
solar heat absorption as a treated megaContinent




